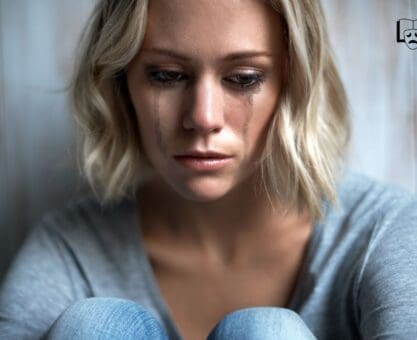
Somatic Healing: How Trauma Lives in the Body
I remember the first time my shoulders unclenched during a simple shaking exercise. It wasn’t dramatic. No cinematic sobbing. Just a tiny relief that felt like a window opening on a stuffy day. That moment shifted how I think about trauma and the body, and it’s why I write about somatic therapy, somatic experiencing, and practical grounding techniques in plain language for people who want real tools.
Why trauma hides in the body (nervous system basics)
Your nervous system doesn’t care that the danger is “over.” It cares whether you feel safe right now. When something scary happens, your body runs a fast survival script: fight, flight, freeze, or collapse. If the moment can’t fully resolve, those trauma responses can stick around as patterns—jumpy sleep, a hair-trigger startle, stomach flips, or classic PTSD symptoms that don’t respond to logic.
“The body keeps the score.” — Bessel van der Kolk
I learned this the annoying way. After a minor car scrape—barely a dent—my jaw clench showed up like an unpaid intern and refused to leave for months. No scary memories. No dramatic story. Just a tight, aching hinge every time I drove, proof my body filed the incident under “still happening.”
This is where body awareness matters. Before you can name an emotion, you can often notice interoceptive sensations: tight chest, clenched jaw, buzzing hands, a throat that won’t swallow. I think of them as flashlights. They point to what the nervous system is bracing against, even when your mind is trying to move on.
Somatic therapy aims at these physiological loops, not just the story. Research reviews report somatic-style interventions often run 1–15 sessions and target bodily regulation directly (see: PMC8276649).
How somatic experiencing and somatic therapy work
I used to think trauma healing was a talking problem. Then my body disagreed—tight jaw, buzzing legs, that “I’m fine” smile glued on like bad tape.
Small sensations, small doses
Somatic experiencing, developed by Peter A. Levine, works on a blunt idea: notice what’s happening inside, let the body finish what it started, and don’t force the story. Instead of replaying the worst day of your life, you track heat, tingling, pressure, shaking, breath changes. The pace is titrated—tiny steps—because flooding people is a great way to get nowhere fast.
“Somatic experiencing offers a way to renegotiate traumatic energy without reliving the whole event.” — Peter A. Levine
Resource orientation and (sometimes) therapeutic touch
A good practitioner keeps you anchored with resource orientation: a steadying image, the feel of your feet, a supportive memory, the chair under your thighs. In some forms of somatic therapy, therapeutic touch may be used with clear consent—think grounding contact, not mystery healing hands.
Why it feels different than talk therapy
Talk therapy can explain your patterns. Somatic experiencing and somatic therapy aim to change the nervous system’s reflexes. Early research shows preliminary positive effects on well-being and affective symptoms, with studies reporting reduced PTSD symptoms, depression, and somatic complaints across trauma types. Sessions vary wildly—sometimes 1, sometimes 15—because bodies don’t read schedules.
Shaking: the overlooked release (step-by-step examples)
I used to think shaking meant “I’m losing it.” Turns out it often means my body is finishing a stress response it never got to complete. In trauma release work, shaking can start as tiny tremors in the calves or hands, then grow—only if it feels safe. Comfort is the rule. Drama isn’t required.
“Small, rhythmic movement often allows the nervous system to offload held energy.” — Dr. Babette Rothschild
What it looks like (and what it isn’t)
Expect subtle, body focused movement: a light bounce, a quiver, a gentle shimmy. If you’re forcing it, you’re doing CrossFit, not nervous regulation.
1–3 minute micro-session (beginner-friendly)
- Warm-up (20 seconds): Feet planted hip-width. Soft knees. One hand on chest, one on belly. In through the nose, out longer.
- Self-check (10 seconds): Rate intensity 0–10. Stay at 3–5. That’s gentle movement, not flooding.
- Shake (60–180 seconds): Start at ankles. Let it travel up. Keep jaw loose. Exhale like you’re fogging a mirror.
- Cool-down (30 seconds): Stop. Press feet into the floor. Name 5 things you see (grounding techniques).
Extra grounding options
- Tense–relax: Squeeze fists 5 seconds, release 10.
- Running water: Hold hands under cool water and track sensation.
Safety: Stop if dizziness, numbness, or panic spikes. If you’re unsure, use a practitioner or a steady partner. Clinical work that includes shaking techniques often runs 1–15 sessions, and that pacing exists for a reason.
Yoga and mindful movement: practical poses and cues
I don’t care how “flexible” you are. If your nervous system is on high alert, fancy poses won’t help. Trauma-sensitive yoga works because it builds structural safety: choice, predictability, and grounding, so body awareness doesn’t feel like a trap. Pairing breath work with movement also nudges parasympathetic activation—your body’s built-in brake pedal.
“Simple, predictable movement gives people permission to feel their body without threat.” — Janice Gates, yoga teacher and trauma specialist
Three poses I keep coming back to
- Child’s pose (containment): knees wide or together, forehead on fists or a pillow. Cue: exhale to soften your belly. If it feels exposing, take puppy pose at the wall instead.
- Cat-cow (spinal release): slow, small range. Cue: inhale to expand the ribs; exhale to round and let the shoulders drop. This is mindful movement plus gentle stretching without forcing anything.
- Legs-up-the-wall (parasympathetic tone): hips can be far from the wall. Cue: let the jaw unclench. If legs tingle, bend knees or prop calves on a chair.
Breath work timing (simple, not heroic)
Use a steady count: inhale 4–6 seconds, exhale 6–8 seconds. Longer exhale signals “safe enough” during trauma processing.
Skip hands-behind-head, deep backbends, or closed-eye cues if they spike you. Keep your gaze soft, name the next move before it happens, and give yourself an exit route—always.

Breath work and grounding techniques you can use anywhere
Panic loves tight spaces: elevators, checkout lines, the “we need to talk” text. My fix isn’t fancy. It’s breath work plus grounding techniques that fit in a pocket.
“Grounding the body re-orients attention away from overwhelming memories toward present safety.” — Dr. Stephen Porges
Micro breath work for nervous regulation
Start with mindful breaths that bias the exhale. Longer exhales nudge nervous regulation in a polyvagal-informed way.
- 4–6–8 breathing: inhale 4–6s, pause 0–2s, exhale 6–8s. Shoulders drop. Jaw unclenches.
- Box breathing: 4s in, 4s hold, 4s out, 4s hold. Use it when your brain won’t stop narrating.
Polyvagal grounding cues (quiet, but effective)
Polyvagal grounding is basically giving your nervous system proof you’re safe. Picture a safe person (real or imagined). Add a slow exhale. Then try gentle humming—vibration can calm the vagal system.
A 90-second reset
60 seconds: count breaths from 1 to 10, restart if you lose track.
30 seconds: sensory check—feel feet in shoes, name 3 sounds, notice temperature on your skin.
If symptoms stay sticky, I pair these with clinical support like EMDR therapy and somatic work. Resources: traumahealing.org, PositivePsychology, and a directory like Somatic Therapy Partners.
Evidence, limitations, and how to choose a practitioner
What the research actually says
I’m cautiously impressed. A 2021 clinical review in PMC reports somatic interventions are linked with reduced PTSD symptoms, less depression, and fewer somatic complaints in several groups (including post traumatic stress presentations). That lines up with field summaries from Somatic Therapy Partners, PositivePsychology, and traumahealing.org: trauma healing often improves when the body gets a vote.
“Research shows somatic interventions can reduce PTSD and related somatic complaints, but approaches vary.” — Clinical research review (2021)
Somatic Experiencing (SE), founded by Peter Levine, has preliminary but promising evidence. I also like pairing somatic therapy with emdr therapy when it’s clinically appropriate—different tools, same nervous system.
Limitations (aka: don’t buy the hype)
Study designs are all over the place: different session counts, mixed methods, small samples. We need more RCTs before anyone claims SE “works for everyone.”
Choosing a practitioner: my non-negotiables
- Verified training: SE via IFSE resources, trauma-sensitive yoga, breathwork safety.
- Clear consent and pacing; “resource-oriented” work to avoid re-traumatization.
- Clinical supervision and scope clarity (especially with dissociation).
- Red flags: instant-cure promises, pushing catharsis, vague plans, no check-ins.
A tiny, real-world routine to start tonight
I don’t trust big “healing plans.” My nervous system hears that and hits snooze. This is small on purpose: micro-practices keep trauma release from feeling like a full-contact sport, and consistency builds safer integration over time.
60-second breath tune-up (4–6–8)
Sit on the edge of the bed. Soft eyes. One hand on your belly if that feels okay. Inhale for 4, hold for 6, exhale for 8. Repeat for one minute. These mindful breaths are boring in the best way—steady input for your body awareness.
2-minute shaking (gentle movement)
Stand. Feet grounded. Knees soft. Shake your arms lightly like you’re flicking water off your fingers. Let it travel to shoulders, ribs, maybe hips. Keep it gentle movement, not a workout. Then stop. Rest. Notice: warmth, tingles, yawns, irritation—whatever shows up.
60–90 second grounding check
Use simple grounding techniques: name 5 things you see, 4 you can touch, 3 you hear. If your mind wanders, good. Come back anyway.
“Short, consistent practices beat sporadic extremes.” — Clinical trauma coach, Laura Mendel
Stopping rules: if you feel dizzy, numb, panicky, or “far away,” stop and orient to the room. Jot two lines after: what you felt, what triggered it. If you have severe dissociation or PTSD symptoms, get practitioner support (start here: ISTSS).
Wild card: a hypothetical—what if the body could talk back?
I want my body awareness to come with subtitles. Because if my shoulders could talk, they’d be rude in the most helpful way.
Me: “Hey, why are you up by my ears again?”
Shoulders: “I’ve been holding this since 2010. You’re welcome.”
Me: “Since 2010? That’s… a long time.”
Shoulders: “Yeah. Also, stop calling it ‘bad posture.’ It’s old alarm.”
That’s the vibe I aim for in trauma release work: curious, a little amused, zero shame. When I treat tension like a cranky coworker instead of a personal failure, my nervous system softens. Then mindful movement actually lands—shaking, slow yoga, breathwork—because I’m not trying to “fix” myself. I’m listening.
“Sometimes humor eases the nervous system enough to let sensation move.” — Somatic practitioner, Maya Rodriguez
Odd metaphors help. A jaw clench can be “a vise.” A tight belly can be “a seatbelt.” My own jaw? It loves to audition for a role as a nutcracker the second I open my inbox. When I notice it and think, “Oh, there you are,” the grip often loosens on its own. Tiny win.
If you want deeper context on why the body keeps receipts, I like this resource: https://traumahealing.org. Next time your body tenses, ask it one question: “How long have you been on duty?”
TL;DR: Trauma can be stored as bodily tension and dysregulated nervous system patterns. Somatic therapy, including shaking, yoga, and breath work, uses body awareness and mindful movement to ease symptoms and support trauma healing.